What Is the PCL?
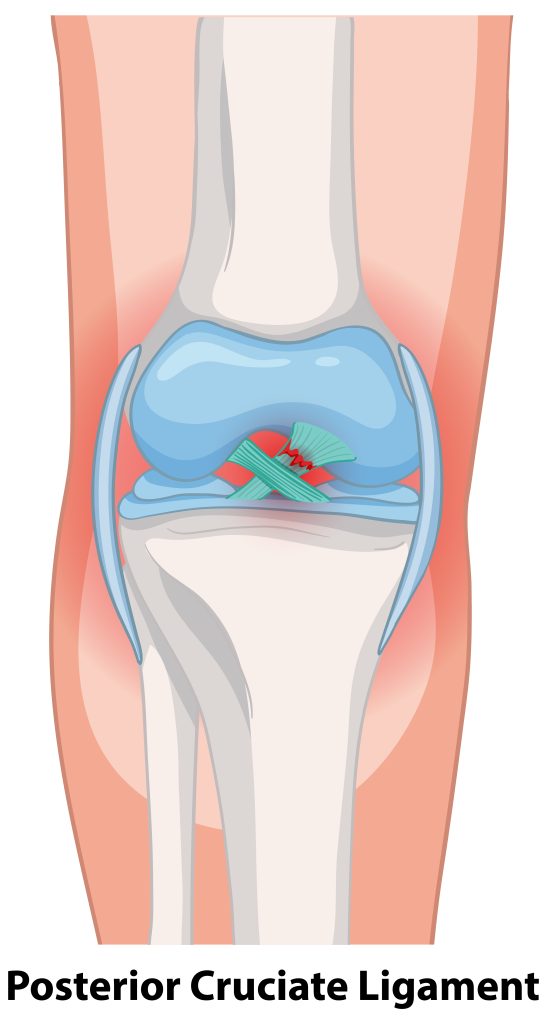
The Posterior Cruciate Ligament (PCL) is one of the key stabilizing ligaments inside the knee joint. Located just behind the ACL, it connects the back of the tibia (shinbone) to the femur (thighbone). As the strongest ligament in the knee, the PCL helps prevent the tibia from shifting too far backward relative to the femur, especially during activities like walking downhill or decelerating quickly.
Although PCL injuries are less common than ACL tears, they can still cause significant instability and dysfunction—particularly if not recognized early or if combined with other ligament damage.
What Causes a PCL Injury?
PCL injuries are typically the result of high-energy trauma or direct impact. Common causes include:
-
A blow to the front of the shin (e.g., a “dashboard injury” during a car accident)
-
Falling hard onto a bent knee
-
Sports accidents involving hyperflexion or twisting
-
High-speed collisions or multi-ligament trauma
PCL injuries may also occur alongside damage to the posterolateral corner, meniscus, cartilage, or other major ligaments (ACL, MCL, LCL), especially in more complex cases.
Symptoms of a PCL Injury
Unlike ACL injuries, which often produce a “pop” and immediate instability, PCL injuries can be more subtle—especially in low-grade tears. Common symptoms include:
-
Pain and swelling, especially behind the knee
-
Bruising over the front of the shin
-
Knee instability, particularly when going down stairs or hills
-
A sense of the knee “slipping” backward
-
Difficulty with sudden stops, pivots, or deceleration
-
Limited range of motion or stiffness
-
Discomfort when walking or bearing weight
Patients sometimes attribute PCL injuries to simple sprains, which is why early evaluation is essential for proper diagnosis and treatment.
How Are PCL Injuries Diagnosed?
At Kerlan Jobe Institute, we use a combination of clinical evaluation and advanced imaging to assess PCL integrity:
-
Posterior drawer test: Assesses backward movement of the tibia
-
Quadriceps active test: Measures tibial shift during quad contraction
-
Dial test: Screens for associated posterolateral instability
-
Gait analysis: Observes for “varus thrust” or abnormal knee motion
We typically confirm the diagnosis with:
-
MRI: Evaluates ligament tears and coexisting injuries
-
Stress X-rays: Measure the functional looseness (posterior tibial translation) compared to the healthy knee
-
CT angiogram (if vascular injury is suspected in high-energy trauma cases)
Grading PCL Injuries
PCL injuries are typically classified by severity:
-
Grade 1: Mild sprain with minimal laxity
-
Grade 2: Partial tear with moderate instability
-
Grade 3: Complete tear with significant instability (often with other ligament damage)
Treatment Options for PCL Injuries
Non-Surgical Management (Grades 1 & 2)
Many isolated PCL injuries—particularly low-grade tears—can be successfully managed without surgery. Non-operative care may include:
-
Functional bracing to prevent backward tibial shift
-
Crutches during early healing
-
RICE protocol (Rest, Ice, Compression, Elevation)
-
Physical therapy focused on strengthening the quadriceps, improving range of motion, and restoring functional stability
Patients are closely monitored through imaging and clinical tests to ensure the ligament is healing in a stable position.
Surgical Reconstruction (Grade 3 or Complex Injuries)
Surgery is typically recommended for:
-
Complete PCL tears (Grade 3)
-
Combined ligament injuries (multi-ligament knee trauma)
-
Chronic instability affecting function or performance
-
Athletes returning to high-demand sports
PCL reconstruction involves replacing the torn ligament with a graft, often using cadaver tissue (allograft) due to the PCL’s size and strength requirements. During surgery:
-
Precise bone tunnels are created in the femur and tibia
-
The graft is tensioned and secured at anatomical attachment sites
-
Any additional ligament or posterolateral corner damage is addressed at the same time
At Kerlan Jobe Institute, our surgeons are highly experienced in advanced PCL reconstruction techniques and manage a high volume of complex knee cases annually.
Recovery Timeline After PCL Surgery
Recovery from PCL reconstruction is structured and progressive. While timelines vary, general expectations include:
-
First 6 weeks:
-
Crutches and brace use
-
Limited weight-bearing to protect the graft
-
Early physical therapy to maintain motion
-
-
Weeks 6–12:
-
Gradual increase in strength and range of motion
-
Controlled weight-bearing and functional movement
-
-
Months 3–6:
-
Advanced neuromuscular training
-
Stationary cycling and low-impact conditioning
-
-
Months 6–9+:
-
Return-to-sport testing
-
Gradual reintegration into sport or high-demand activities
-
Full recovery may take 9 to 12 months, especially when combined ligament injuries are involved.
Why Trust Kerlan Jobe Institute for PCL Injuries?
PCL injuries are often underdiagnosed, undertreated, or mismanaged—especially when part of a complex knee injury. At Kerlan Jobe Institute, we offer:
-
Expert-level diagnostic precision
-
Experience in single- and multi-ligament reconstruction
-
Customized rehab protocols
-
Comprehensive surgical and non-surgical options
Our goal is to restore knee strength, confidence, and long-term joint health—whether you’re a competitive athlete or an active individual eager to return to your lifestyle.