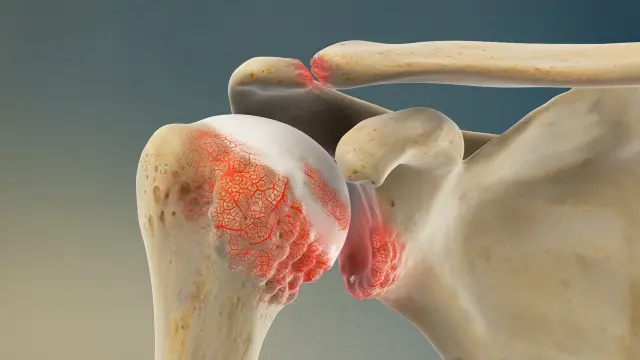
AC (Acromioclavicular) joint arthritis is a form of osteoarthritis that affects the small joint where the clavicle (collarbone) meets the acromion of the scapula (shoulder blade). This joint is responsible for allowing arm elevation and shoulder rotation. Over time, wear and tear can lead to the breakdown of cartilage, resulting in joint inflammation, pain, and limited shoulder motion.
Causes and Risk Factors
-
Natural aging process and degenerative changes
-
Repetitive shoulder use or overhead lifting
-
Prior trauma or AC joint separation
-
Weightlifting and contact sports (e.g., football, rugby)
-
Occupations requiring frequent lifting or pushing
-
Previous surgery involving the shoulder or clavicle
Symptoms
-
Localized pain on the top of the shoulder
-
Pain when reaching across the body (e.g., putting on a seatbelt)
-
Tenderness over the AC joint
-
Swelling or a visible bump at the AC joint
-
Discomfort during push-ups, bench press, or overhead lifting
-
Limited range of motion, especially at the end range of elevation
Diagnosis
-
Physical exam: focal tenderness at the AC joint, pain with cross-body adduction test
-
X-rays typically show:
-
Joint space narrowing
-
Bone spurs (osteophytes)
-
Cyst formation or sclerosis
-
-
MRI may reveal cartilage loss and inflammation
-
Diagnostic lidocaine injection into the AC joint can confirm the source of pain
Treatment
Non-Surgical Treatment
-
NSAIDs to reduce inflammation and pain
-
Activity modification (avoiding aggravating movements)
-
Ice and topical analgesics
-
Physical therapy to:
-
Improve shoulder mechanics
-
Reduce strain on the AC joint
-
-
Corticosteroid injection into the AC joint for longer-lasting relief
Surgical Treatment
-
Indicated for persistent or severe symptoms despite conservative treatment
-
Common procedures:
-
Distal clavicle excision (also known as the Mumford procedure): removal of a small portion of the clavicle to eliminate bone-on-bone contact
-
Performed arthroscopically or via a mini-open approach
-
-
Usually a same-day outpatient procedure
Recovery Outlook
-
Many patients achieve long-term relief through non-surgical care
-
After distal clavicle excision:
-
Sling use for a few days to a week
-
Return to desk work in 1–2 weeks
-
Full recovery within 6–8 weeks
-
Return to weightlifting or high-demand activity typically in 3 months
-
Why Kerlan Jobe Institute?
Our orthopedic specialists at Kerlan Jobe Institute have deep expertise in managing AC joint arthritis using both conservative and minimally invasive surgical techniques. We focus on helping each patient return to pain-free motion and daily function.